Edit, Download, and Sign the BlueCross BlueShield Illinois Claim Form
Form
eSign
Add Annotation
Share Form
How do I fill this out?
To properly fill out this claim form, start by providing your personal information as the insured/subscriber. Ensure that all sections are accurately filled out per the instructions provided on the reverse side. Double-check the information for accuracy before submission.
How to fill out the BlueCross BlueShield Illinois Claim Form?
1
Complete every item on the claim form.
2
Provide accurate patient and insured information.
3
Indicate the type of treatment received.
4
Attach the necessary itemized bills.
5
Sign and date the form before submitting.
Who needs the BlueCross BlueShield Illinois Claim Form?
1
Individuals seeking reimbursement for medical expenses incurred.
2
Parents filing claims for children's medical treatments.
3
Retired individuals accessing benefits after employment.
4
Employees looking for insurance coverage verification.
5
Healthcare providers needing authorization for treatments.
How PrintFriendly Works
At PrintFriendly.com, you can edit, sign, share, and download the BlueCross BlueShield Illinois Claim Form along with hundreds of thousands of other documents. Our platform helps you seamlessly edit PDFs and other documents online. You can edit our large library of pre-existing files and upload your own documents. Managing PDFs has never been easier.
Edit your BlueCross BlueShield Illinois Claim Form online.
You can edit this PDF on PrintFriendly by first uploading your document to our platform. Utilize our editing tool to modify any section of the claim form. Once finished, save your edits and download the updated copy for submission.
Add your legally-binding signature.
Signing the PDF on PrintFriendly is straightforward; just use our signature feature after editing. You can add your digital signature directly on the form. After signing, download the signed document for your records.
Share your form instantly.
Sharing the PDF via PrintFriendly is simple and efficient. Once your document is edited, use our sharing options to send it directly to your contacts. This feature enhances collaborative efforts for claim submission.
How do I edit the BlueCross BlueShield Illinois Claim Form online?
You can edit this PDF on PrintFriendly by first uploading your document to our platform. Utilize our editing tool to modify any section of the claim form. Once finished, save your edits and download the updated copy for submission.
1
Upload the PDF claim form to PrintFriendly.
2
Select the section you wish to edit and make necessary changes.
3
Review all modifications for accuracy.
4
Use the signature tool if you need to sign the document.
5
Download the edited PDF when finished.

What are the instructions for submitting this form?
To submit this form, ensure that all fields are accurately filled and that itemized bills are attached. You can send your completed claim form via mail to BlueCross BlueShield of Illinois at P.O. Box 660603, Dallas, TX 75266-0603. For quick submission, consider faxing your documents to the dedicated claims fax number provided on the form or use any available online submission options offered by your insurance provider.
What are the important dates for this form in 2024 and 2025?
Ensure to submit your claim form within the specified timeframes outlined by BlueCross BlueShield. Important deadlines for 2024 and 2025 can vary, so always check directly with your provider. This will help avoid delays in processing your claims.

What is the purpose of this form?
The purpose of this form is to provide a structured method for insured individuals to request coverage for medical expenses incurred. By filling out this claim form correctly, users enable BlueCross BlueShield of Illinois to assess their claims accurately. This facilitates a smoother reimbursement process for treatments received.
Tell me about this form and its components and fields line-by-line.
- 1. Insured/Subscriber Name: Full name of the insured or subscriber.
- 2. Group Number: Insurance group identification number.
- 3. Insurance Identification Number: Unique identifier from the insurance card.
- 4. Address: Mailing address of the insured.
- 5. Patient's Full Name: Full name of the patient receiving treatment.
- 6. Patient's Date of Birth: Date of birth of the patient.
- 7. Treatment Type: Type of treatment received.
- 8. Diagnosis: Details on symptoms or diagnosis.
- 9. Signature: Insured's signature to authorize the claim.
What happens if I fail to submit this form?
Failure to submit this form may result in delays or denial of your health benefits claims. It's crucial to ensure all required fields are completed accurately. Incomplete submissions can complicate the processing and reimbursement of your medical expenses.
- Delays in Benefits Processing: Incomplete or incorrect claims can result in significant delays.
- Claim Denials: Claims submitted without all necessary information are likely to be denied.
- Increased Out-of-Pocket Costs: Neglecting submission requirements can lead to higher out-of-pocket expenses.
How do I know when to use this form?
- 1. After Medical Treatment: Use this form immediately after receiving a covered medical service.
- 2. To File for Reimbursement: When you need to be reimbursed for out-of-pocket expenses.
- 3. In the Case of Multiple Treatments: If you've received different types of treatments or procedures.
Frequently Asked Questions
How do I start filling out this claim form?
Begin by downloading the form and reading the instructions carefully to understand what information is required.
Can I edit the PDF before submitting?
Yes, PrintFriendly allows you to edit the PDF to fill out the necessary details.
What information do I need to provide?
You will need to provide information about the insured, the patient, and the type of treatment received.
How do I attach itemized bills?
Ensure to have your itemized bills ready, and follow the instructions for attaching them to the claim form.
Is there a limit to the types of treatments I can claim?
Typically, each claim form should be used for one type of treatment to avoid confusion.
What happens if my claim is denied?
If a claim is denied, details will usually be provided in your Explanation of Benefits document.
How do I know where to send my claim form?
The address for submission is listed at the end of the claim form.
What if I have additional questions about the claim process?
Contact customer service or refer to the FAQ section on the BlueCross BlueShield website.
Can I save my form locally after editing?
Yes, you can download the edited form to your device for your records.
How do I ensure my information remains confidential?
PrintFriendly guarantees a user-friendly experience while maintaining the integrity of your PDF documents.
Related Documents - BCBS Claim Form
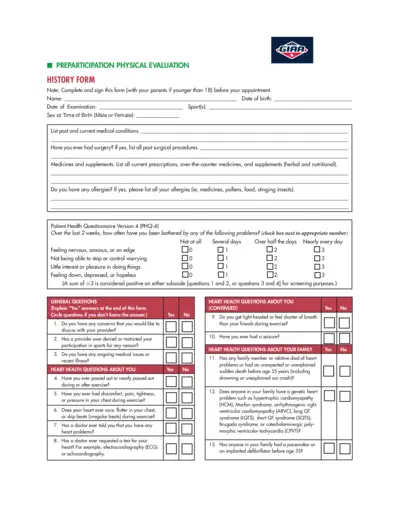
Preparticipation Physical Evaluation Form
The Preparticipation Physical Evaluation Form is used to assess the physical health and fitness of individuals before they participate in sports activities. It covers medical history, heart health, bone and joint health, and other relevant medical questions.
Health Insurance Tax Credits Guide 2015
This document provides a comprehensive guide on health insurance and premium tax credits for the 2015 tax year. It explains the tax filing rules, eligibility criteria, and detailed instructions for claiming and reporting premium tax credits. Essential for individuals who bought health insurance through the ACA Marketplaces.
TSP-77 Partial Withdrawal Request for Separated Employees
The TSP-77 form is used by separated employees to request a partial withdrawal from their Thrift Savings Plan account. It includes instructions for completing the form, certification, and notarization requirements. The form must be filled out completely and submitted along with necessary supporting documents.
Ray's Food Place Donation Request Form Details
This file contains the donation request form for Ray's Food Place. Complete the general information section and follow the guidelines to submit your donation request at least 30 days in advance. The form includes fields for organization details and donation specifics.
Pastoral Ministry Evaluation Form for Board of Elders
This evaluation form is designed for the Board of Elders to assess and provide feedback on a pastor's ministry. It aims to offer affirmation and identify areas for improvement. The form covers preaching, worship leading, pastoral care, administration, and more.
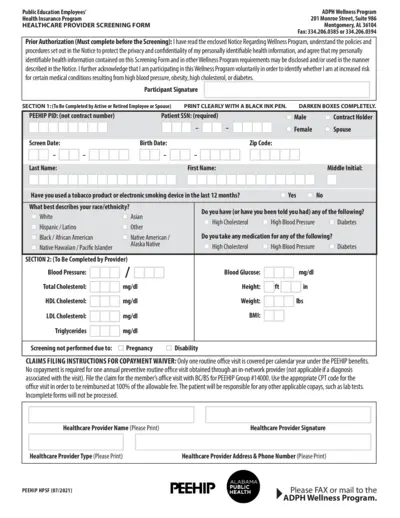
Health Provider Screening Form for PEEHIP Healthcare
This file contains the Health Provider Screening Form for PEEHIP public education employees and spouses. It includes instructions on how to fill out the form for wellness program participation. The form collects personal, medical, and screening details to assess wellness.
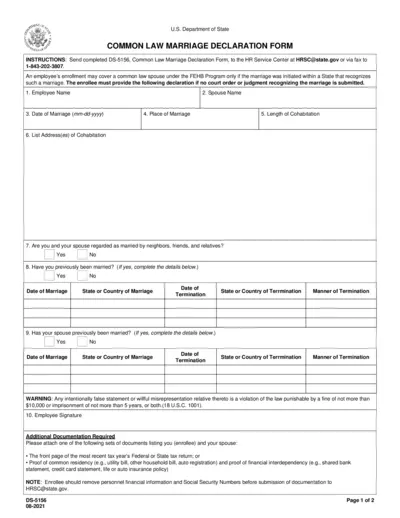
Common Law Marriage Declaration Form for FEHB Program
This form is used to declare a common law marriage for the purpose of enrolling a spouse under the Federal Employees Health Benefits (FEHB) Program. It requires personal details, marriage information, and additional documentation. Submission instructions and legal implications are included.
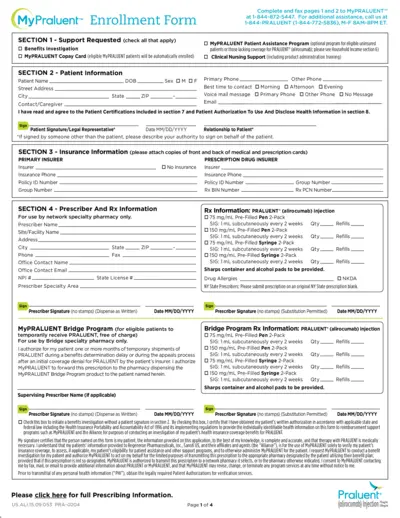
MyPRALUENT™ Enrollment Form Instructions and Details
This document provides comprehensive instructions and details for enrolling in the MyPRALUENT™ program, including benefits, patient assistance, and clinical support. It outlines the required patient, insurance, and prescriber information, as well as the steps for treatment verification and household income documentation.
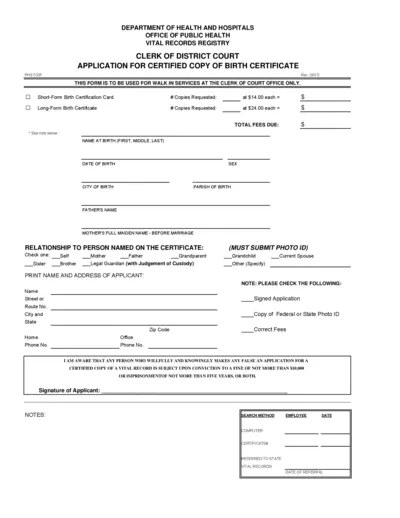
Application for Certified Copy of Birth Certificate
This form is used to request a certified copy of a birth certificate from the Clerk of Court Office. It includes details about the applicant, the person named on the certificate, and requires a photo ID and the correct fee. This form is only for walk-in services.
Torrance Memorial Physician Network Forms for Patients 18+
This file contains important forms for patients 18 years and older registered with Torrance Memorial Physician Network. It includes patient registration, acknowledgment of receipt of privacy practices, and financial & assignment of benefits policy forms. Complete these forms to ensure your medical records are up-to-date and to understand your financial responsibilities.
Vodafone Phone Unlocking Guide: Steps to Unlock Your Phone
This guide from Vodafone provides a step-by-step process to unlock your phone. Learn how to obtain your unlock code by filling out an online form. Follow the instructions to complete the unlocking process.
Texas Automobile Club Agent Application Form
This file is the Texas Automobile Club Agent Application or Renewal form, which must be submitted within 30 days after hiring an agent. The form includes fields for agent identification, moral character information, and requires signature from both the agent and an authorized representative of the automobile club. Filing fees and submission instructions are also provided.

